Psychedelic Harm Reduction and Integration (PHRI): A Clinician's Guide
Write your awesome label here.
A client mentions, near the end of a session, that she took mushrooms with a friend over the weekend. Not in a trial. Not at an Oregon service center. In her friend's living room, because she had read that psilocybin might help with the depression that two SSRIs hadn't touched. Then she watches your face to see what happens next.
The short version: Psychedelic Harm Reduction and Integration (PHRI) is an evidence-informed clinical stance for working with clients who use psychedelics, regardless of whether you ever administer a substance. It combines non-judgmental harm reduction with structured integration, meaning the work of making sense of an experience after the fact. PHRI is not a protocol or a credential. It is a way to apply what you already know, within your existing scope.
What PHRI actually is
The framework has a specific origin. In 2021, Ingmar Gorman, Elizabeth Nielson, and colleagues published Psychedelic Harm Reduction and Integration: A Transtheoretical Model for Clinical Practice in Frontiers in Psychology, defining PHRI as a transtheoretical, transdiagnostic approach to working with patients who are using or considering using psychedelics in any context, without the clinician providing the substance. It combines harm reduction psychotherapy, the relational stance of psychedelic-assisted therapy, mindfulness-based approaches, and psychodynamic listening.
It is a way to bring competencies you already have to a situation your training did not address. The “transtheoretical” label is doing real work: whether you practice from a CBT, psychodynamic, ACT, or somatic base, PHRI describes a stance you layer on top of it, not a modality you have to adopt instead.
It is a way to bring competencies you already have to a situation your training did not address. The “transtheoretical” label is doing real work: whether you practice from a CBT, psychodynamic, ACT, or somatic base, PHRI describes a stance you layer on top of it, not a modality you have to adopt instead.
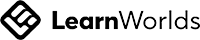
- Harm reduction is the stance you take toward use that is already happening or being considered: meet it without moralizing, reduce risk where you can, and stay in the room.
- Integration is the work of helping a client metabolize what will happen or happened into something usable, durable, and connected to the rest of their life.
Why you will meet these clients whether or not you seek them
Harm reduction without the moralizing
Integration is the work. It is not an add-on.
What PHRI asks of the clinician
The shape of the market
Where this connects
Frequently asked questions
What is Psychedelic Harm Reduction and Integration (PHRI)?
PHRI is a transtheoretical clinical model, defined by Gorman and colleagues in 2021, for working with clients who use or are considering psychedelics, without the clinician administering anything. It combines harm reduction psychotherapy with integration, the work of making meaning afterward, and applies across diagnoses and therapeutic orientations.
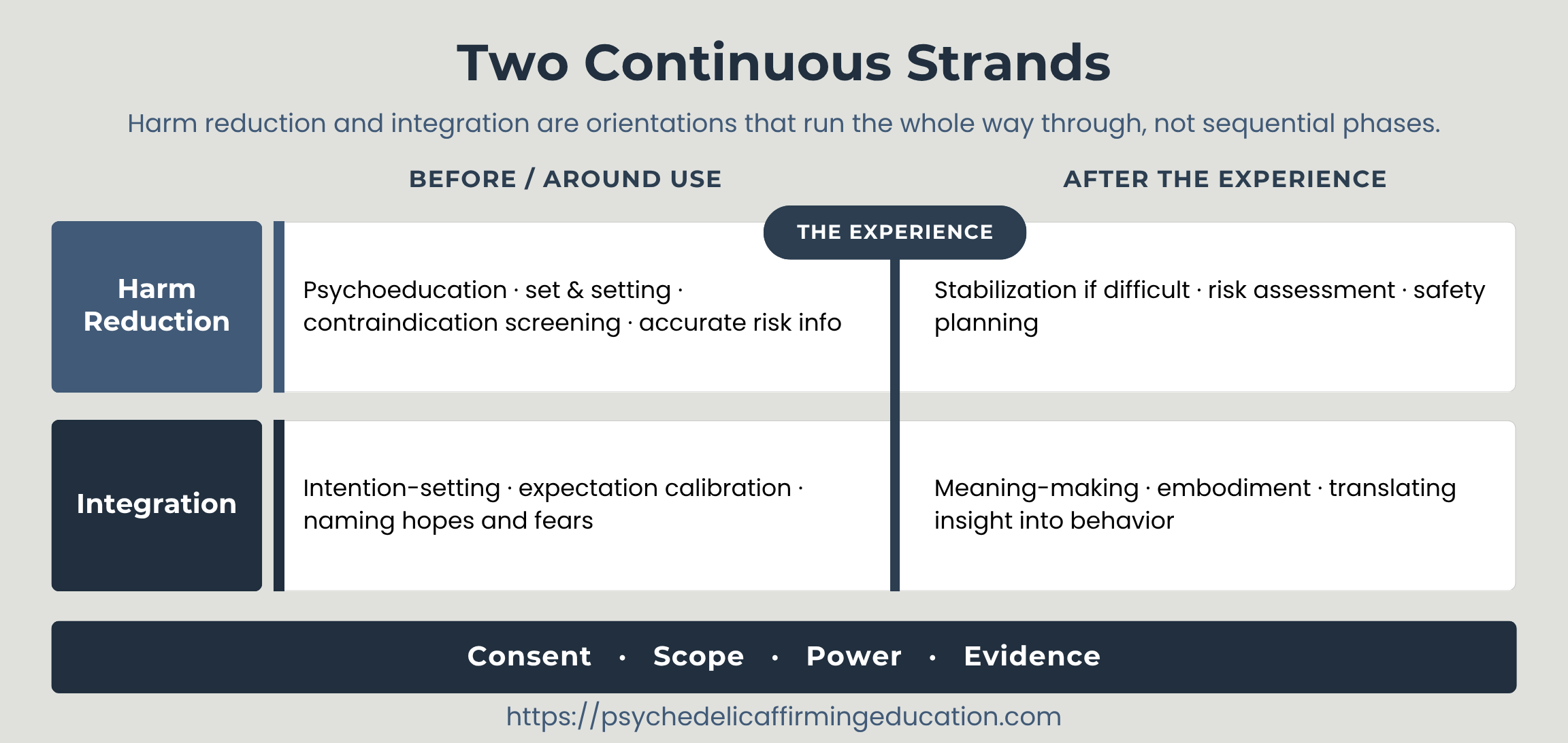
How is PHRI different from psychedelic-assisted therapy?
In psychedelic-assisted therapy, the clinician administers a substance within a legal protocol and supports the client through the experience. PHRI involves no administration. It is the model for the far more common situation where a client uses psychedelics independently and brings that experience into ordinary therapy for harm reduction and integration support.
Do I need special training or a license to practice PHRI?
No special license is required, because PHRI does not involve administering any substance. It draws on competencies licensed clinicians already have. What it asks for is specific competence: understanding harm reduction, integration practices, contraindications, scope-of-practice limits, and the heightened power dynamics involved. Continuing education in these areas is an ethical responsibility, not a legal requirement.
Is supporting a client’s illegal psychedelic use within my scope?
You can support a client in making meaning of an experience they chose to have, and you can reduce harm by discussing risk honestly. You cannot direct, recommend, or facilitate illegal use. The distinction is between responding to what a client brings you and instigating or arranging use, and articulating that line clearly is part of practicing PHRI responsibly.
What does the evidence actually show about integration?
Integration is a near-universal component of psychedelic trials and is supported by strong clinical consensus, but no published study has yet isolated it as a variable. Definitions, practice guidelines, and validated measurement scales now exist, while outcome research does not. The claim that integration drives lasting change is clinically grounded, not yet experimentally proven.
How do I become someone clients will disclose psychedelic use to?
Disclosure follows safety. Clients read your reactions long before they test you with the topic, so a non-judgmental, accurate, non-moralizing stance toward substances signals that the conversation is safe to have. Avoiding visible alarm, knowing the basics, and asking open questions about use all increase the likelihood of disclosure.
Author: Peter H. Addy, PhD, LPC (Oregon), LMHC (Washington), is a licensed psychotherapist, clinical supervisor, and former Yale School of Medicine postdoctoral researcher in psychedelic science. He is the founder of Psychedelic Affirming Education, an NBCC-approved continuing education provider (ACEP No. 7579). PAE’s accuracy and editorial standards: https://psychedelicaffirmingeducation.com/ce-policies
Pages
Policy Pages
Created with